




فېمور بوينى سۇنۇشلىرى فېمور بوينى سۇنۇشلىرىنىڭ %50 نى ئىگىلەيدۇ. فېمور بوينى سۇنۇش كېسىلىگە گىرىپتار بولغان قېرى بولمىغان بىمارلارغا ئادەتتە ئىچكى جەھەتتىن تىكلەش داۋالىشى تەۋسىيە قىلىنىدۇ. قانداقلا بولمىسۇن، ئوپېراتسىيەدىن كېيىنكى ئاسارەتلەر، مەسىلەن، سۇنۇقنىڭ بىرلەشمەسلىكى، فېمور بېشىنىڭ نېكروزلىنىشى ۋە فېمور بوينىنىڭ قىسقىرىشى كلىنىكىلىق ئەمەلىيەتلەردە كۆپ ئۇچرايدۇ. ھازىر، كۆپىنچە تەتقىقاتلار فېمور بوينى سۇنۇشلىرىنى ئىچكى جەھەتتىن تىكلىگەندىن كېيىن فېمور بېشىنىڭ نېكروزلىنىشىنىڭ ئالدىنى ئېلىشقا مەركەزلەشكەن، فېمور بوينىنىڭ قىسقىرىشى مەسىلىسىگە ئانچە دىققەت قىلىنمايدۇ.
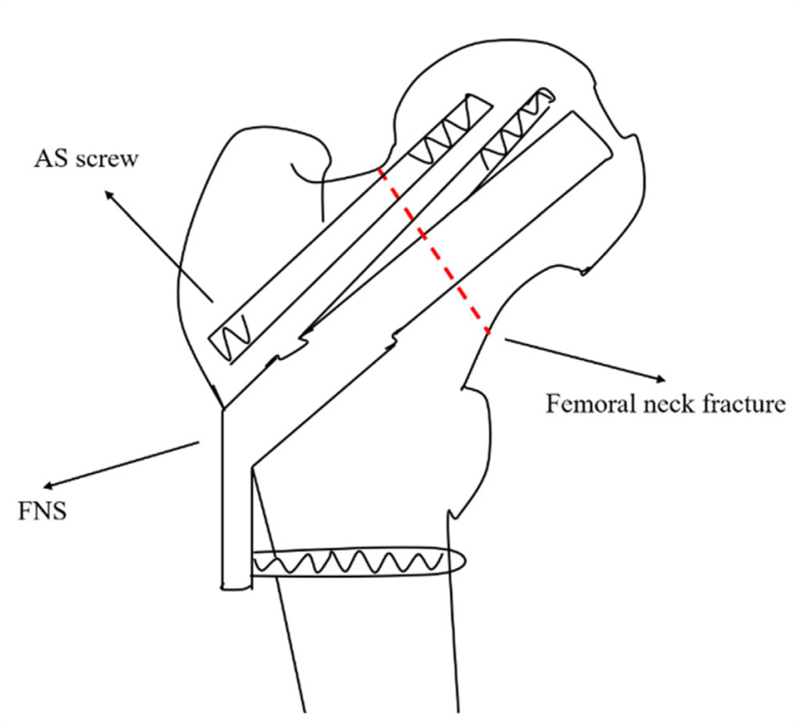
ھازىر، ئۈچ دانە كانۇللىق ۋىنت، FNS (فېمورال بويۇن سىستېمىسى) ۋە دىنامىك يانپاش ۋىنتلىرىنى ئىشلىتىش قاتارلىق، فېمورال بوينىنىڭ ئىچكى جەھەتتىن بېكىتىلىشىنىڭ ئالدىنى ئېلىش ۋە ئوق يۆنىلىشىدە سىقىلىش ئارقىلىق بىرىكمەسلىكنىڭ ئالدىنى ئېلىشنى مەقسەت قىلىدۇ. قانداقلا بولمىسۇن، كونترول قىلىنمىغان ياكى ھەددىدىن زىيادە سىيرىلىپ بېسىم قىلىش مۇقەررەر ھالدا فېمورال بوينىنىڭ قىسقىرىشىغا ئېلىپ كېلىدۇ. بۇنى نەزەردە تۇتۇپ، فۇجيەن ئەنئەنىۋى جۇڭگو تېبابىتى ئۇنىۋېرسىتېتى قارمىقىدىكى ئىككىنچى خەلق دوختۇرخانىسىنىڭ مۇتەخەسسىسلىرى، فېمورال بوينىنىڭ ئۇزۇنلۇقىنىڭ سۇنۇقنىڭ ساقىيىشى ۋە يانپاش ئىقتىدارىدىكى مۇھىملىقىنى كۆزدە تۇتۇپ، فېمورال بوينىنىڭ سۇنۇقىنى بېكىتىۋېلىش ئۈچۈن FNS بىلەن بىرلەشتۈرۈلگەن «قىسقارتىلىشقا قارشى ۋىنت» ئىشلىتىشنى تەكلىپ قىلدى. بۇ ئۇسۇل ئۈمىدۋار نەتىجىلەرنى كۆرسەتتى، ھەمدە بۇ تەتقىقات «ئورتوپېدىيە ئوپېراتسىيەسى» ژۇرنىلىنىڭ ئەڭ يېڭى سانىدا ئېلان قىلىندى.
ماقالىدە ئىككى خىل «قىسقارتىشقا قارشى بۇراما» تىلغا ئېلىنغان: بىرى ئۆلچەملىك كانۇلالىق بۇراما، يەنە بىرى قوش يىپلىق لايىھەلىك بۇراما. قىسقارتىشقا قارشى بۇراما گۇرۇپپىسىدىكى 53 قاپنىڭ ئىچىدە پەقەت 4 قاپتا قوش يىپلىق بۇراما ئىشلىتىلگەن. بۇ قىسمەن يىپلىق كانۇلالىق بۇراما ھەقىقەتەن قىسقارتىشقا قارشى تۇرۇش ئۈنۈمىگە ئىگەمۇ دېگەن سوئالنى كەلتۈرۈپ چىقىرىدۇ.
قىسمەن يىپلىق كانۇلداتلانغان ۋىنتلار ۋە قوش يىپلىق ۋىنتلار بىرلىكتە تەھلىل قىلىنىپ، ئەنئەنىۋى FNS ئىچكى بېكىتىش بىلەن سېلىشتۇرۇلغاندا، نەتىجىلەر شۇنى كۆرسەتتىكى، 1 ئايلىق، 3 ئايلىق ۋە 1 يىللىق كۆزىتىش نۇقتىلىرىدا، قىسقارماسلىق ۋىنت گۇرۇپپىسىدىكى قىسقارۇش دەرىجىسى ئەنئەنىۋى FNS گۇرۇپپىسىدىكىگە قارىغاندا كۆرۈنەرلىك دەرىجىدە تۆۋەن بولۇپ، ستاتىستىكىلىق ئەھمىيەتكە ئىگە. بۇ سوئالنى كەلتۈرۈپ چىقىرىدۇ: بۇ تەسىر ئۆلچەملىك كانۇلداتلانغان ۋىنتتىنمۇ ياكى قوش يىپلىق ۋىنتتىنمۇ؟
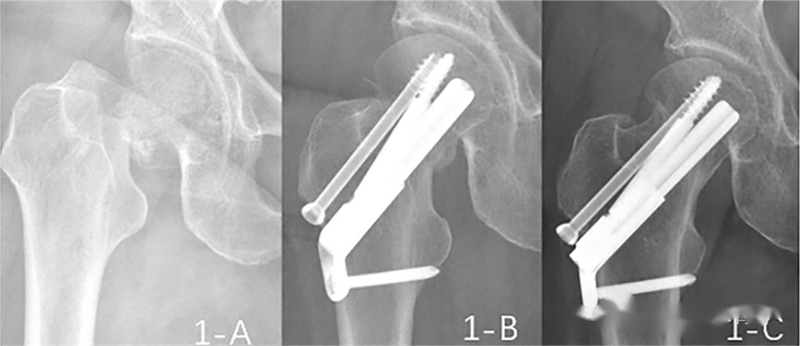
بۇ ماقالىدە قىسقارتىشقا قارشى ۋىنتلارغا مۇناسىۋەتلىك 5 ئەھۋال كۆرسىتىلدى، تېخىمۇ يېقىندىن تەكشۈرگەندە، قىسمەن يىپلىق كانۇليالىق ۋىنت ئىشلىتىلگەن 2- ۋە 3- ئەھۋاللاردا، ۋىنتنىڭ چېكىنىشى ۋە قىسقارغانلىقى كۆرۈنەرلىك بولغانلىقىنى كۆرگىلى بولىدۇ (ئوخشاش نومۇر بىلەن بەلگىلەنگەن رەسىملەر ئوخشاش ئەھۋالغا ماس كېلىدۇ).

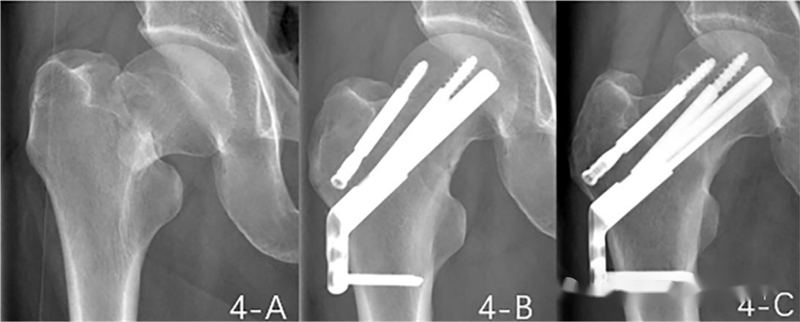


ئەھۋال رەسىملىرىگە ئاساسلانغاندا، قوش يىپلىق ۋىنتنىڭ قىسقارماسلىقتىكى ئۈنۈمى ناھايىتى روشەن. كانۇليالىق ۋىنتلارغا كەلسەك، بۇ ماقالىدە ئۇلار ئۈچۈن ئايرىم سېلىشتۇرۇش گۇرۇپپىسى بېرىلمىگەن. قانداقلا بولمىسۇن، بۇ ماقالىدە فېمۇر بوينىنىڭ ئىچكى قىسمىنى بېكىتىش توغرىسىدا قىممەتلىك قاراشلار بېرىلگەن بولۇپ، فېمۇر بوينىنىڭ ئۇزۇنلۇقىنى ساقلاشنىڭ مۇھىملىقىنى تەكىتلەيدۇ.
ئېلان قىلىنغان ۋاقىت: 2024-يىلى 9-ئاينىڭ 6-كۈنى





